















 497 656
497 656

reporting of this subpathology. The clinical utility of IDC is
arguably greater if incorporation of this pathological feature
into existing clinical models were to improve the prediction
of biochemical andmetastatic relapse. On the basis of recent
evidence from several large cohort studies, it can be
concluded that IDC is an independent prognostic factor
for recurrence, and even mortality
[2,5]. IDC also frequently
coexists with another subpathology, cribriform architecture
(CA); both lesions are believed to have comparable
prognostic impact and independently improve on prognos-
tic stratification compared to the sole use of clinical indices
[5]. However, it remains to be seen if IDC and CA are
predictive markers for the efficacy of treatment intensifica-
tion in the era of second-generation antiandrogen agents
(eg, enzalutamide, abiraterone) and taxane chemotherapy.
In their review, Porter et al note the persistence of IDC in
nearly 60% of tumor specimens following exposure to prior
androgen suppression or chemotherapy
[6]. This is provoc-
ative, as it suggests that IDC is intrinsically resistant to
systemic therapies, and novel treatment intensification
protocols may be required to improve outcomes in patients
whose tumors harbor IDC-CA.
How do we begin to explain the biology underlying the
aggression associated with IDC-CA lesions? A recent study of
genomic profiling of matched primary-metastatic tumors
revealed a close relationship between tumor clones within
the metastases and the IDC subpathology, suggesting that
IDC may be the nidus of prometastatic tumor clones
[8] .[(Fig._1)TD$FIG]
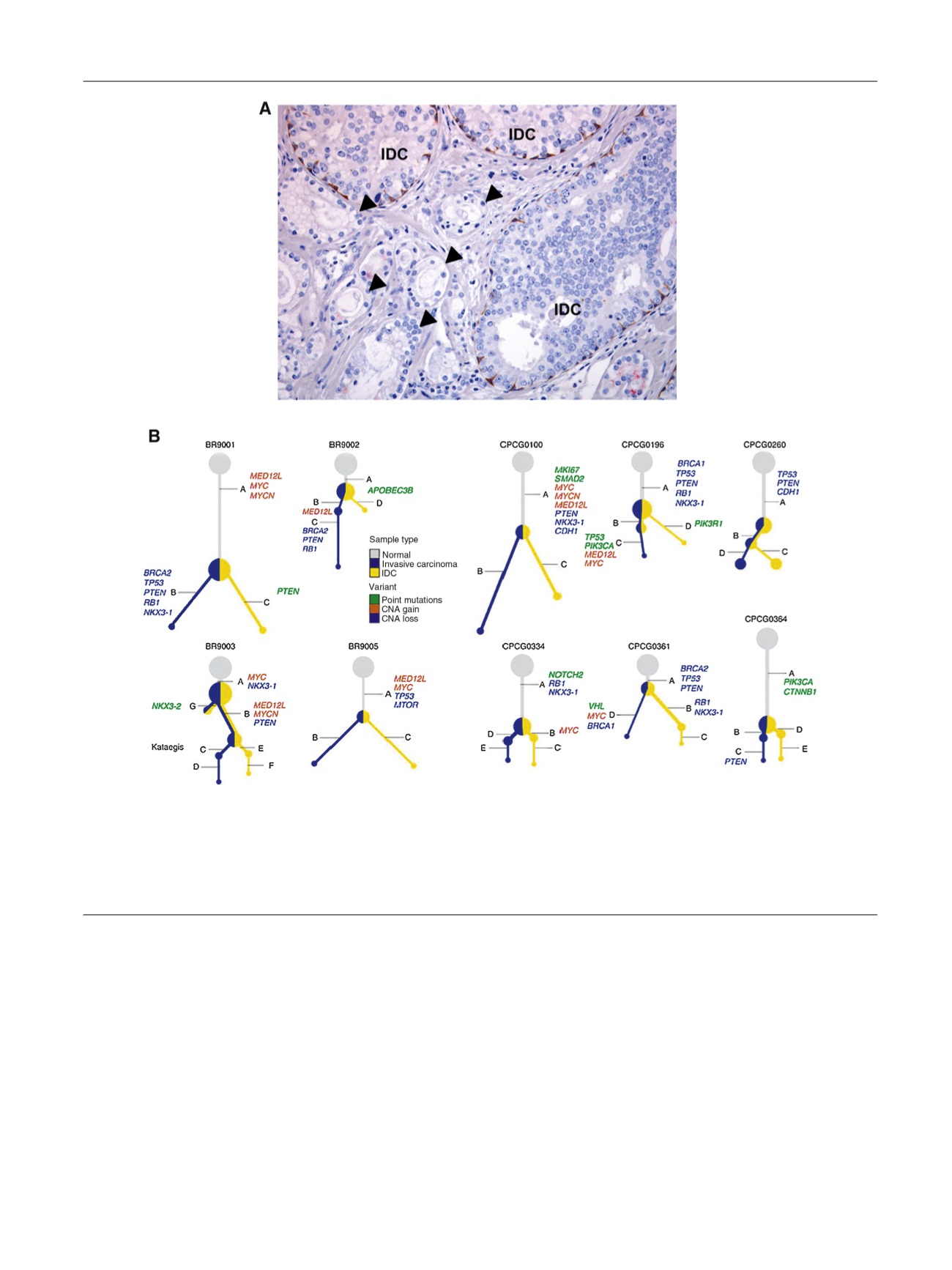
Fig. 1 – Molecular pathological hallmarks of intraductal carcinoma (IDC)–positive prostate cancer. (A) Histomorphology of IDC (labeled) as characterized
by a rim of basal cells (brown color) outlining the antecedent prostate duct, distended by carcinoma cells displaying a cribriform architecture. The
remaining glands (closed arrows) lacking basal cells are glandular adenocarcinoma. (B) Subclonal reconstruction of
BRCA2
-mutant (BR samples) and
sporadic (CPCG samples) prostate cancers from microdissected IDC and invasive carcinoma components. Both lesions originate from the same clonal
ancestry, with subsequent branching to multiple subspecies.
MED12L
amplification was predominant among
BRCA2
-mutant tumors; sporadic IDC-
positive tumors had a higher frequency of
PIK3CA
mutations compared to The Cancer Genome Atlas localized prostate cancer cohort
[9] .Adapted from
Taylor et al
[9] .CNA = copy number aberration.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 4 9 6 – 4 9 8
497