















 608 656
608 656

critical question arises: Why have we not seen more TE
materials make it into the clinic? There are probably two
primary reasons. (1) With very few exceptions, the majority
of preclinical models did not investigate the pathological
aspects of the stricture, so links between models and the
clinic are missing
[9] .(2) Transferring preclinical knowledge
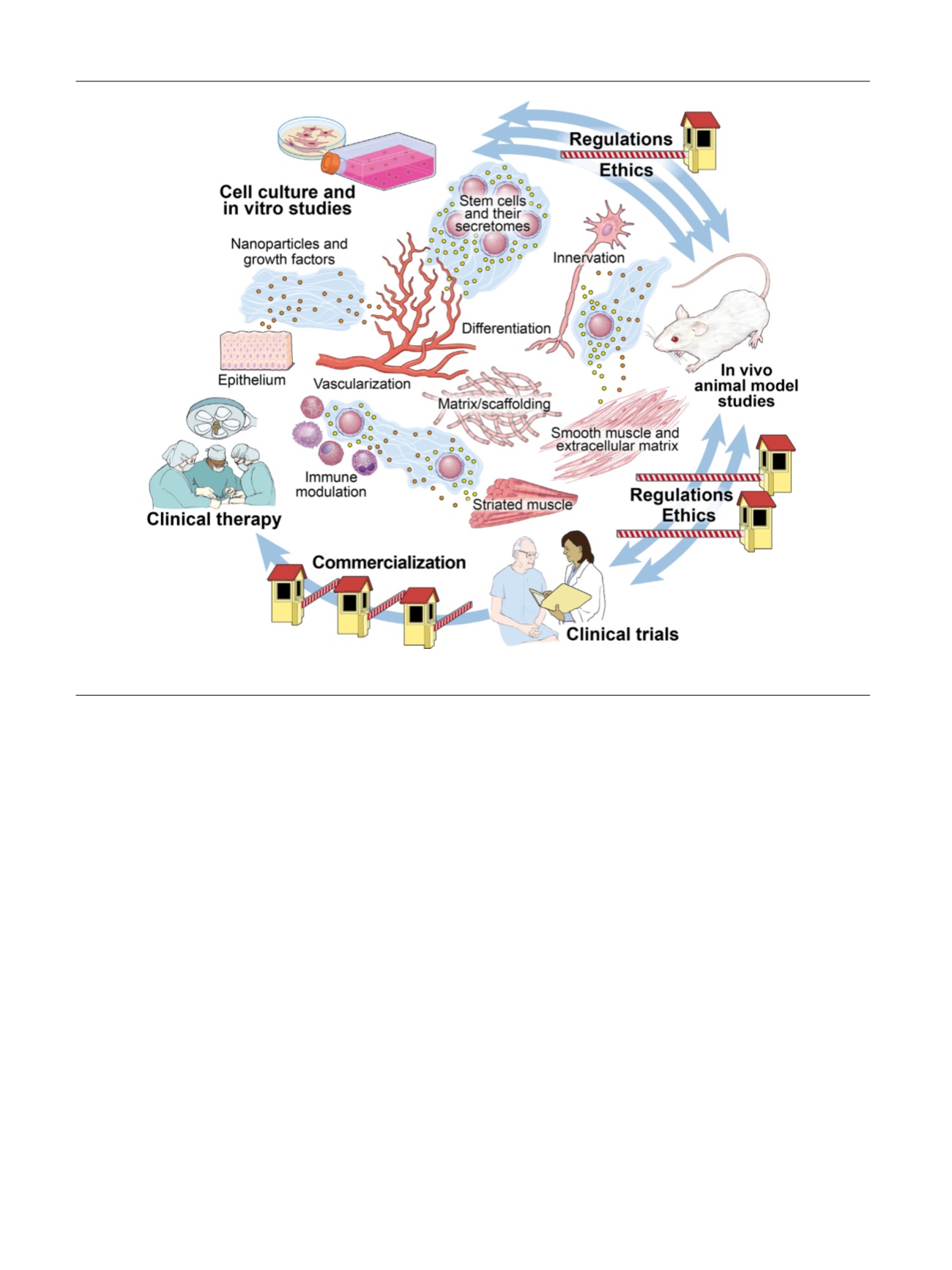
into clinical therapy is a difficult process
[10,11], starting
with cell culture and in vitro studies and continuing with in
vivo animal model studies, clinical trials, and commerciali-
zation, with regulatory oversight at all stages
( Fig. 1 [12]).
The technical requirements for producing acellular TE
materials are challenging. In addition, although TE is
performed at controlled manufacturing sites according to
the principles of Good Manufacturing Practice, various
problems may arise, for example, during the transport of
matrices to other locations. Such issues become even more
challenging when seeded matrices are used
[13].
At present, multiple regulatory experiments related to
emerging therapies using human cells are under way, and
approaches differ across countries
[14] .In Europe, the
process is constrained by regulatory challenges because of
legislation in the individual countries within the EU that
are regulated by the European Medicines Agency. In the
USA, regulations are quite different from those in the EU.
The FDA classifies human cells, tissues, and cellular- and
tissue-based products (HCT/Ps) into three broad categories
[15] :(1) HCT/Ps that fall under section 361 of the US Public
Health Service Act (termed
361s
) are minimally manipu-
lated and used clinically in a homologous manner; (2) HCT/
Ps that fall under section 351 of the US Public Health Service
Act (termed
351s
) are either more than minimally
manipulated or used in a nonhomologous manner; and
(3) combination products.
The meta-analysis performed by Versteegden et al
[4]illustrates the limitations of preclinical efforts to find the
best possible material for urethral reconstruction and the
major difficulties in taking the next step into clinical
studies. Conducting a successful clinical study is a time-
consuming and expensive undertaking. The authors not
only highlight the importance of designing solid basic
research but also point out the importance of farsighted
planning so that the data fulfill legal requirements and
ultimately achieve an approved therapeutic option
[16].
Conflicts of interest:
The author has nothing to disclose.
References
[1]
Chapple C, Andrich D, Atala A, et al. SIU/ICUD Consultation on urethral strictures: The management of anterior urethral stricture disease using substitution urethroplasty. Urology 2014;83:S31–47.[(Fig._1)TD$FIG]
Fig. 1 – Tissue engineering and regenerative medicine: bench to bedside in urology. Reprinted from
[12]with permission from Elsevier.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 6 0 7 – 6 0 9
608