















 611 656
611 656

1.
Introduction
First described in 1976, percutaneous nephrolithotomy
(PCNL) has gained an established role in the contemporary
surgical management of urolithiasis
[1,2]. Both European
Urology Association and American Urological Association
guidelines recommend PCNL as the treatment option for
larger renal calculi
[3,4].
The PCNL procedure includes several steps: percutane-
ous puncture of a renal calyx, tract dilatation, nephroscopy,
and stone fragmentation and removal
[5]. Among these
steps, obtaining safe and appropriate access to the kidney
represents one of the most difficult, and can ultimately
impact the outcomes of the procedure
[6]. Fluoroscopy and
ultrasound, alone or combined, are the methods most often
used to guide puncture of the renal collecting system
[7]. However, access techniques based on these methods
remain suboptimal
[8]. Moreover, concerns related to
radiation exposure when fluoroscopy is used have been
raised
[9].
We recently described experimental use of a novel
visual-assisted navigation system in a porcine model using
real-time electromagnetic sensors to allow kidney puncture
for PCNL
[10]. Here we report the first use of this device in
humans and describe in detail the surgical technique and
analyze early clinical outcomes.
2.
Patients and methods
2.1.
Study design
This was a prospective proof-of-concept phase 1 study according to the
IDEAL criteria
[11]. All procedures were performed by a single staff
surgeon (E.L.) at the CUF Department of Urology of Braga Hospital (Braga,
Portugal), which is a tertiary academic medical center. All patients gave
their written informed consent to test our navigation system for renal
colleting system puncture after the risks, benefits, and alternatives were
discussed. Institutional review board approval was obtained before the
start of the study. Patients were specifically informed that this was first
clinical application of this novel system. The primary endpoint was the
clinical applicability of the system for PCNL. Secondary endpoints were
assessment of accuracy (in terms of time to successful puncture and
number of attempts for successful puncture) and safety (in terms of
puncture-related complications).
2.2.
Patient selection criteria
Inclusion criteria for patient selection were: age older than 18 yr; stone
in the renal pelvis; stone size 2.5 cm; and Guy’s stone score of 1–2
[12].
Exclusion criteria were: obese patient (body mass index [BMI]
>
30 kg/m
2
); lower calyx fully engaged with stones; bilateral stones,
solitary kidney, renal insufficiency, anatomic renal anomalies, stone size
>
2.5 cm, and Guy’s stone score of 3–4
[12] .2.3.
Perioperative management
Patients underwent standard preoperative anesthesia testing. A
computed tomography (CT) urogram with three-dimensional (3D)
reconstruction was also obtained. Patients with negative urine cultures
were treated with a single prophylactic dose of a broad-spectrum
antibiotic.
2.4.
Instrumentation
The commercially available Aurora EMT system (Northern Digital,
Waterloo, Canada) was used to track the catheter and needle tip inside
the ureteral and kidney calyx. This navigation system comprises the
following components
( Fig. 1 ):
(1) A planar, low-intensity, and varying electromagnetic field generator
that establishes a tracking volume.
(2) Two sensor interface units (SIUs) that act as analog-to-digital
converters and amplifiers of the electrical signals from the sensors to
a system control unit (SCU). The SIUs decrease the possibility of
electromagnetic interference in the operating room. The SCU
transmits spatial data to a computer for subsequent processing
and navigation using the software described below.
(3) One Chiba needle (18G/180 mm) and one ureteral catheter of
1.1 mm in diameter and 2 m in length. Both include an Aurora EMT
sensor with five degrees of freedom at its tip.
(4) 3DPuncture software (EMT kidney and ureter percutaneous access
software) for surgical guidance that was developed specifically for
this work using C++ and VTK (The Visualization ToolKit). The
software gathers and processes information from different equip-
ment needed for PCNL puncture: images from the videoureteror-
enoscope, and the orientation and position of the needle and
catheter EMT sensors. It allows the surgeon to choose the correct
needle orientation in real time.
2.5.
Technique
The accompanying video illustrates the technology and provides a step-
by-step description of the procedure. Under general anesthesia, the
patient is placed in the supine position to allow a combined approach
with flexible ureterorenoscopy and percutaneous nephroscopy. The
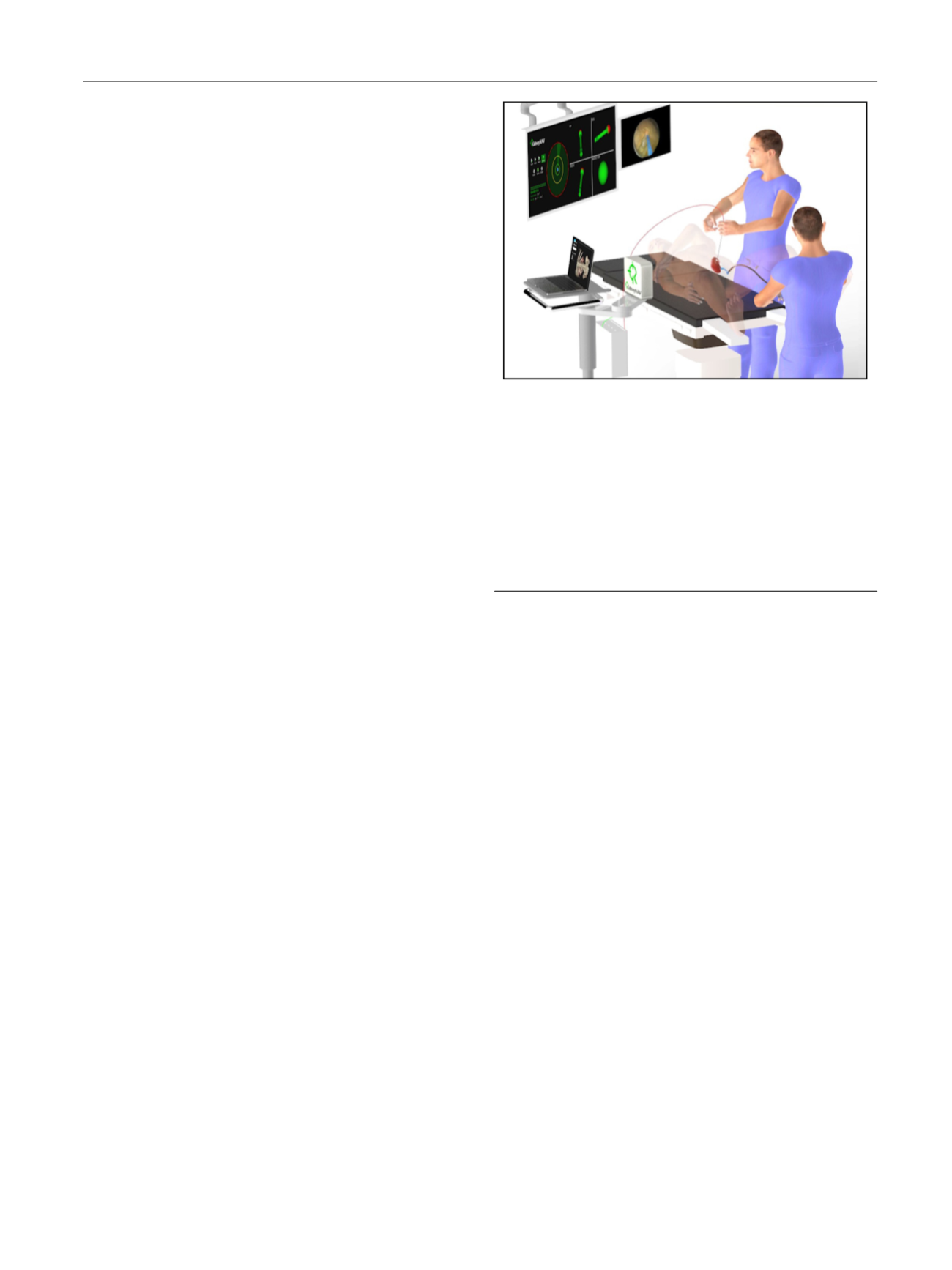
[(Fig._1)TD$FIG]
Fig. 1 – Surgical set-up for puncture of the renal collecting system using
electromagnetic sensors. A research group from the University of Minho
(Braga, Portugal) has patented this new navigation system. The
technology consists of the following components: (1) software for
surgical guidance developed specifically for this work, which acts as a
control station by gathering and processing information from different
equipment needed for puncture for percutaneous nephrolithotomy; (2)
an electromagnetic field generator placed on the opposite side of the
puncture, close to the patient; (3) one 18G needle and one ureteral
catheter, both with an electromagnetic sensor on the tip; (4) a monitor
with a four-view 3D representation of the trajectory orientation and
position of the needle and catheter; and (5) a monitor displaying the
ureterorenoscopy video image.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 6 1 0 – 6 1 6
611