















 612 656
612 656

generator is placed near the patient (outside the surgical field) to create
the electromagnetic field for tracking the position of the catheter and
needle sensors. Then a cystoscope (model 27035BA, Karl Storz,
Tuttlingen, Germany) is inserted for identification of the ureteral
meatus, and a hydrophilic guidewire (model AE0N35, Terumo, Shibuya,
Tokyo) is inserted through it. A digital videoureterorenoscope (Karl Storz
model 11278VSK) is inserted, guided by the hydrophilic guidewire, up to
the renal pyelocaliceal system. No ureteral access sheath is used. After
removing the guidewire, a ureteral catheter with electromagnetic sensor
is inserted through the working channel of the digital videoureteror-
enoscope. Under ureteroscopy visualization, the surgeon selects the
ideal calyx for percutaneous access, and places the ureteral catheter with
the electromagnetic sensor in the fornix of the calyx.
An ultrasound scan is used to verify that the renal puncture track is
not obstructed by any unintended anatomical structure. The selected
calyx is punctured using an 18G needle with an electromagnetic sensor
on the tip of the stylet. The access is guided in real time by images
observed on the monitor
( Fig. 2). Once the needle tip is inserted into the
desired calyx the proper calyceal access is confirmed ureteroscopically,
and minor adjustments are made under endoscopic visualization.
To obtain the working tract for PCNL, the inner stylet containing the
electromagnetic sensor is removed and a guidewire is inserted, followed
by balloon dilatation and sheath placement under direct ureteroscopy
visualization. The entire process is performed without fluoroscopy, and
is only monitored using the digital videoureterorenoscope image.
Finally, the entire PCNL procedure is performed under ureteroscopy
visualization, as described by others
[13].
3.
Results
3.1.
Study population
Ten patients were enrolled in the study. The median age was
47.1 yr (30–63), median BMI was 22.85 kg/m
2
(19–28.3),
and median stone size was 2.13 cm (1.5–2.5 cm). All stones
were in the renal pelvis. The Guy’s stone score was 1 in nine
cases and 2 in one case.
3.2.
Outcomes
The ten punctures of the collecting system were success-
fully completed. The median time to successful puncture
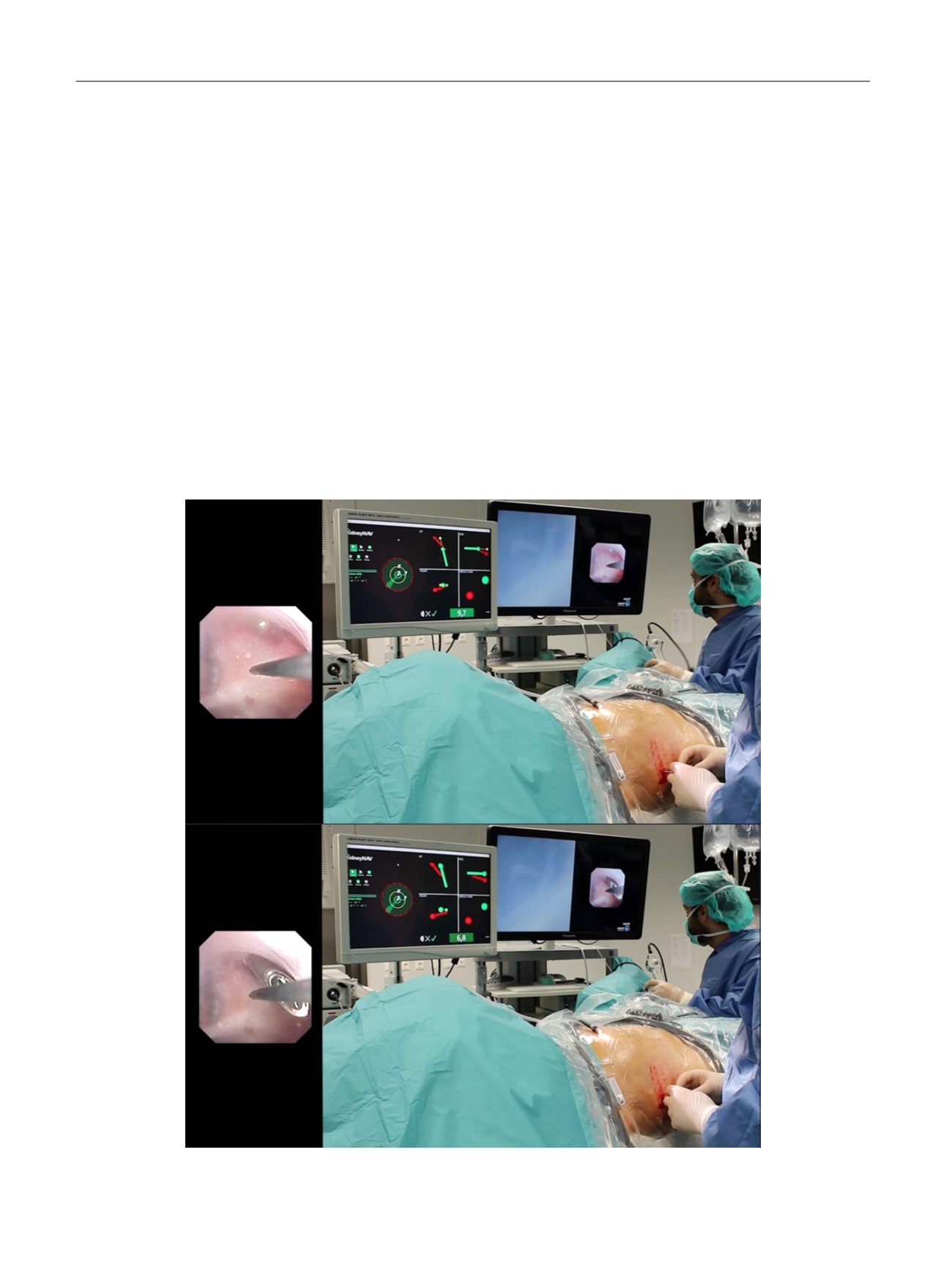
[(Fig._2)TD$FIG]
Fig. 2 – Guided by the three-dimensional navigation software on the monitor and confirmed simultaneously by ureterorenoscope images, the surgeon
performs puncture of the lower calyx during human percutaneous nephrolithotomy.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 6 1 0 – 6 1 6
612