















 618 656
618 656

1.
Introduction
Preservation of erectile function is closely related to outcome
satisfaction for men undergoing curative treatment for
prostate cancer
[1,2] .The ability to alter rates of erectile
function after prostatectomy was founded on a functional
anatomic approach. This method was pioneered by Dr.
Patrick Walsh to systematically nominate and test anatomic
sources to identify and preserve periprostatic structures via
surgical means
[3,4] .This ultimately gave rise to the classical
nerve-sparing radical prostatectomy and its subsequent Veil
of Aphrodite sparing adaptations designed to address the
wide variation in nerve anatomy
[4,5] .However, the cause of
erectile dysfunction (ED) after radiotherapy is less clear.
The etiology of ED is multifactorial, and includes
psychogenic, endocrine, and direct nerve disruptions, among
others
[6] .However, vascular etiologies for ED appear
predominant in prostate cancer survivors after radiotherapy
[7–9] .Two primary reasons have limited progress in the
adoption of a functional anatomic approach using radiother-
apy: (1) the routine use of computed tomography (CT)
imaging to delineate the prostate, which is unable to identify
critical vascular elements (in comparison to magnetic
resonance imaging [MRI]); and (2) older radiotherapeutic
techniques and planning software that were unable to spare
the dose to nearby structures. With the increasing role of MRI
in the management of prostate cancer
[10], we developed a
novel functional anatomic approach termed ‘‘vessel-sparing
radiotherapy’’. Prior studies have assessed the role of sparing
radiation to the penile bulb or erectile tissue of the corpus
cavernosum (CC)
[11–15]; however, sparing of other critical
vascular elements has not been systematically undertaken.
Here we report 5-yr patient-reported erectile function
preservation rates and long-term tumor control outcomes
from a phase 2 trial of vessel-sparing radiotherapy.
2.
Patients and methods
2.1.
Patients and staging
Through aninstitutionalreviewboard–approvedprotocol(NCT02958787),
144menweretreatedwithvessel-sparingradiotherapyattheUniversityof
Michigan in a prospective phase 2 clinical trial from 2001 to 2009. All
patients provided written informed consent before registration.
Men aged 18 yr with prostate adenocarcinoma were eligible if they
had cT1c–T3a disease, Gleason score 6–10, Eastern Cooperative
Oncology Group performance status score
<
2, and no prior pelvic
radiotherapy or definitive surgery for prostate cancer. Patients were
required to have biopsy-proven clinically localized prostate cancer, able
to undergo an MRI of the prostate with contrast, and have an
International Index of Erectile Function (IIEF-5) score of 16. The IIEF
score of 16 was chosen so that all men in the study could be evaluable for
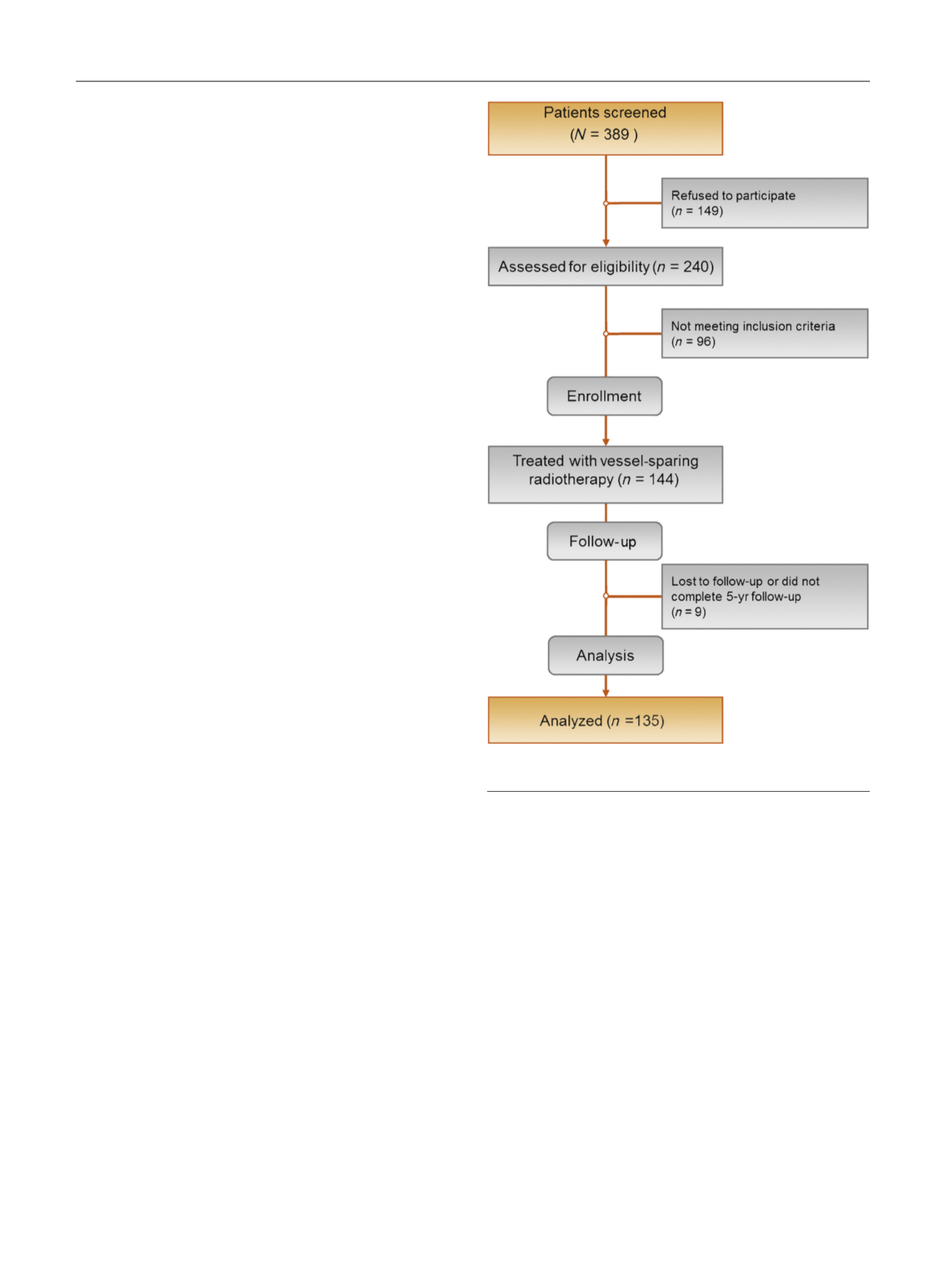
declines in erectile function after treatment. Of patients treated with
vessel-sparing radiotherapy, 135 were followed for a minimum of 5 yr
and form the study cohort
( Fig. 1 ).
2.2.
Treatment
Radiotherapy treatment was risk-adapted in that low-risk and select
intermediate-risk patients were generally treated with intensity-modu-
lated radiotherapy (IMRT) alone to75.6 Gy (range, 75.6–79.2 Gy) in 1.8-Gy
daily fractions. A subset of intermediate-risk and high-risk patients
received IMRT plus supplemental low-dose rate (LDR) permanent
brachytherapy with
125
I to a prescription dose of 110 Gy, followed by
IMRT to 45 Gy. Pelvic lymph nodes were treated to 45 Gy for all high-risk
patients. Androgen deprivation therapy (ADT) was prescribed at the
discretion of the treating physician for a duration of 6 mo, typically for
intermediate-risk and high-risk patients.
The vessel-sparing technique has previously been described by our
group
[3,16]. MRI T2 sequences in all planes (axial, coronal, and sagittal)
were obtained with a pelvic coil using a slice thickness of 5 mm. The
proximal CC was delineated on the axial and coronal T2 MRI. In addition,
an MRI angiogram was obtained to define the internal pudendal artery
(IPA). The goal was to deliver the prescribed radiotherapy dose to the
prostate with maximal sparing of the bilateral CC and IPA. The data sets
were registered to the planning CT scan using mutual information
software. The registration methodology and target delineation for
critical erectile structures have been described previously
[3,16] .Dose
constraint goals are listed in the Supplementary material.
2.3.
Patient assessment and endpoints
Before initiating radiotherapy, patients were evaluated using two
patient-reported questionnaires, as well as physician-interrogated
[(Fig._1)TD$FIG]
Fig. 1 – Consolidated Standards of Reporting Trials (CONSORT) diagram.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 6 1 7 – 6 2 4
618