















 604 656
604 656

may perform adequately and may be a valid alternative.
Clearly, randomized controlled clinical trials are needed to
clarify this issue.
4.1.
Application of cells
There is no consensus on the potential beneficial effects of
cell seeding of tissue engineered constructs for the
urogenital system. For tissue engineering of the bladder,
the addition of cells did not give an overall beneficial effect
on tissue regeneration
[27], while others claim that cells are
required for urethra repair of constructs
>
0.5 cm
[28]. For
urethra tissue engineering, the inclusion of cells signifi-
cantly reduced side effects in preclinical studies for both full
(
p
= 0.001) and inlay (
p
= 0.003) defects. In other, less
comprehensive systematic reviews, a similar outcome
regarding the effectiveness of the addition of cells was
shown
[29,30]. For full defects, cell addition has more added
value, whichmay be explained by the fact that cells can only
infiltrate from the two urethra edges, while in inlay repair
cell ingrowth can also occur from the sides, boosting cell
coverage.
The effects of cell addition on functionality and study
completion were not significant, regardless of surgical
procedure. This may be caused by the short follow-up
period underestimating long-term complications, such as
complete strictures. Meta-analysis of clinical studies
showed no significant effect of cells for any of the outcome
measures. Consequently, the use of cells for the repair of
urethra in the clinic remains debatable.
4.2.
Type of biomaterial
Meta-analysis showed no differences in estimated proba-
bilities for the different materials in most of the conditions,
with the exception of synthetic materials showing better
estimated probabilities than natural materials in full
circumferential repair without cells regarding side effects.
For inlay repair in preclinical studies, synthetic materials
did not perform as well as in full repair, but only a limited
number of studies was reported.
Decellularized materials were used in the vast majority
of clinical studies. This may be related to the experience
with decellularized materials in other fields of tissue
engineering, such as skin tissue engineering
[31] .Which
type of biomaterial is superior to the current state of the art
remains to be established.
4.3.
Selection of animal species
The choice of animal species is often based on financial
issues, experience of the researchers, ethical arguments and
practical restrictions
[32–34] .An evidence-based approach
can aid in selection of the most appropriate model. In this
review, differences between treatment were not notably
influenced by the choice for rabbit or dog; however, a higher
statistical power would strengthen this claim.
4.4.
Clinical relevance and limitations of preclinical and clinical
studies
Quality of the experimental designs and reporting of
preclinical studies was generally low. Proper control groups,
such as sham operation groups and standard treatment
groups, were often lacking. Instead, the experimental
material without cells was generally considered the control.
In addition, outcome measures and drop-outs were not
specifically reported for each animal, complicating data
interpretation. Also, representativeness of presented data
was often not mentioned. This may have hampered clinical
translation of these preclinical findings. To improve this, all
design parameters and outcomes should be specifically
documented for individual animals similar to patients in
clinical studies. The ‘‘Gold standard publication checklist to
improve the quality of animal studies’’ by Hooijmans et al
[35]would be helpful for the design and reporting of
preclinical studies.
Another limitation for the level of evidence provided by
the preclinical studies is the use of healthy animals, in
which a created defect is immediately closed, compared to
patients with a history of stricture, lichen sclerosis or
hypospadias. From the patients in clinical studies 75% had
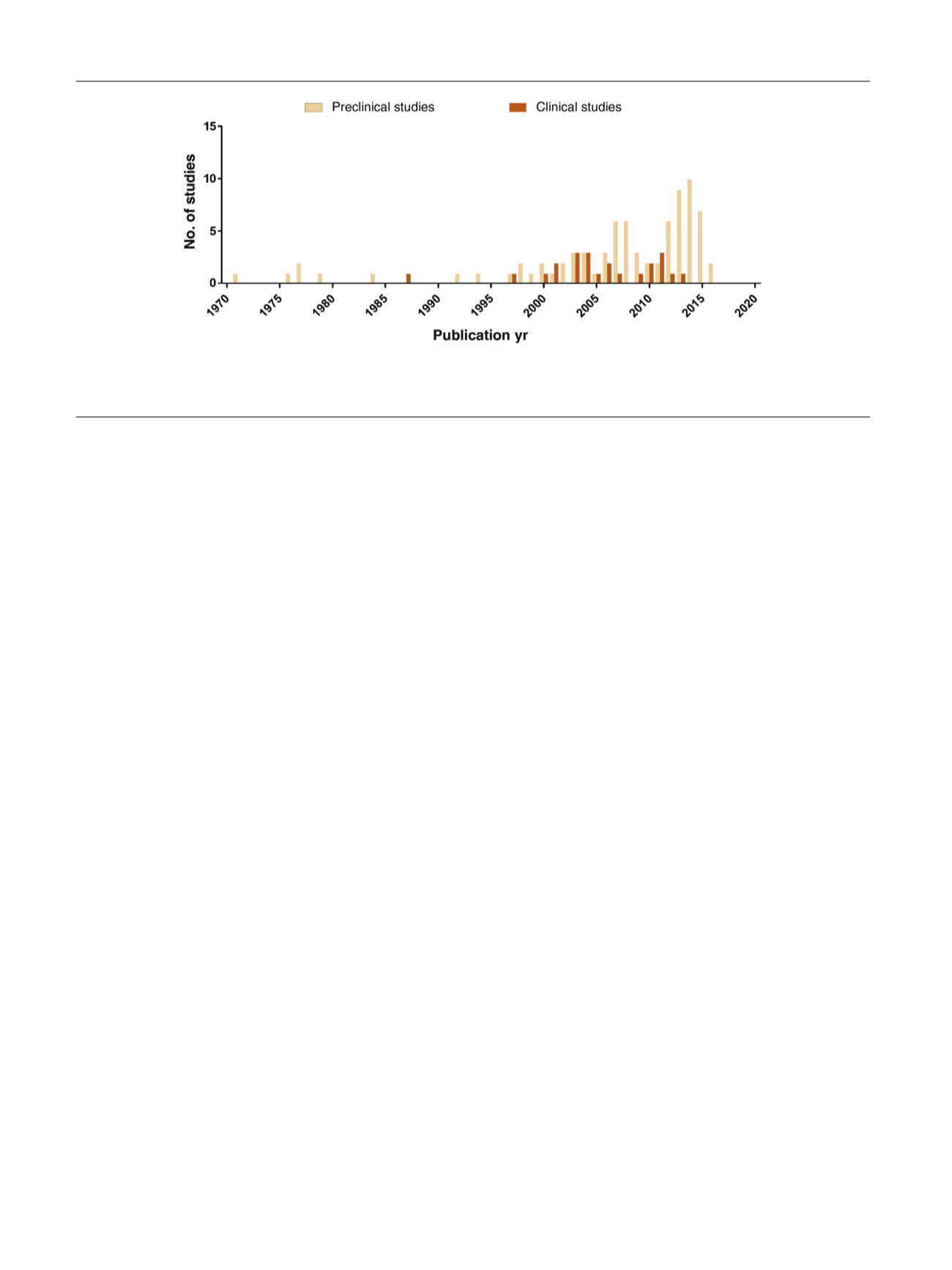
[(Fig._4)TD$FIG]
Fig. 4 – Number of publications per year for preclinical and clinical studies included in this systematic review. After several single studies between
1971 and 1994, the number of publications increased. Peaks in both clinical and preclinical studies were seen around 2005–2008 and again between
2012–2015.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 5 9 4 – 6 0 6
604