















 603 656
603 656

without reintervention and without being lost in follow-up.
Most patients had a history of failed repairs using
conventional techniques, while healthy animals were used.
As randomized clinical studies were lacking, for example,
comparison with standard treatments (free skin graft or
buccal mucosa urethroplasty)
[3], no direct comparisons
with current clinical practice could be made. Available
literature about complex two-stage urethroplasty shows
complication-free rates, functionality, and study comple-
tion of approximately 62%, 67%, and 36%
[26], similar to the
outcome of tissue engineered urethras (based on point
estimates). This suggests that tissue engineered urethras
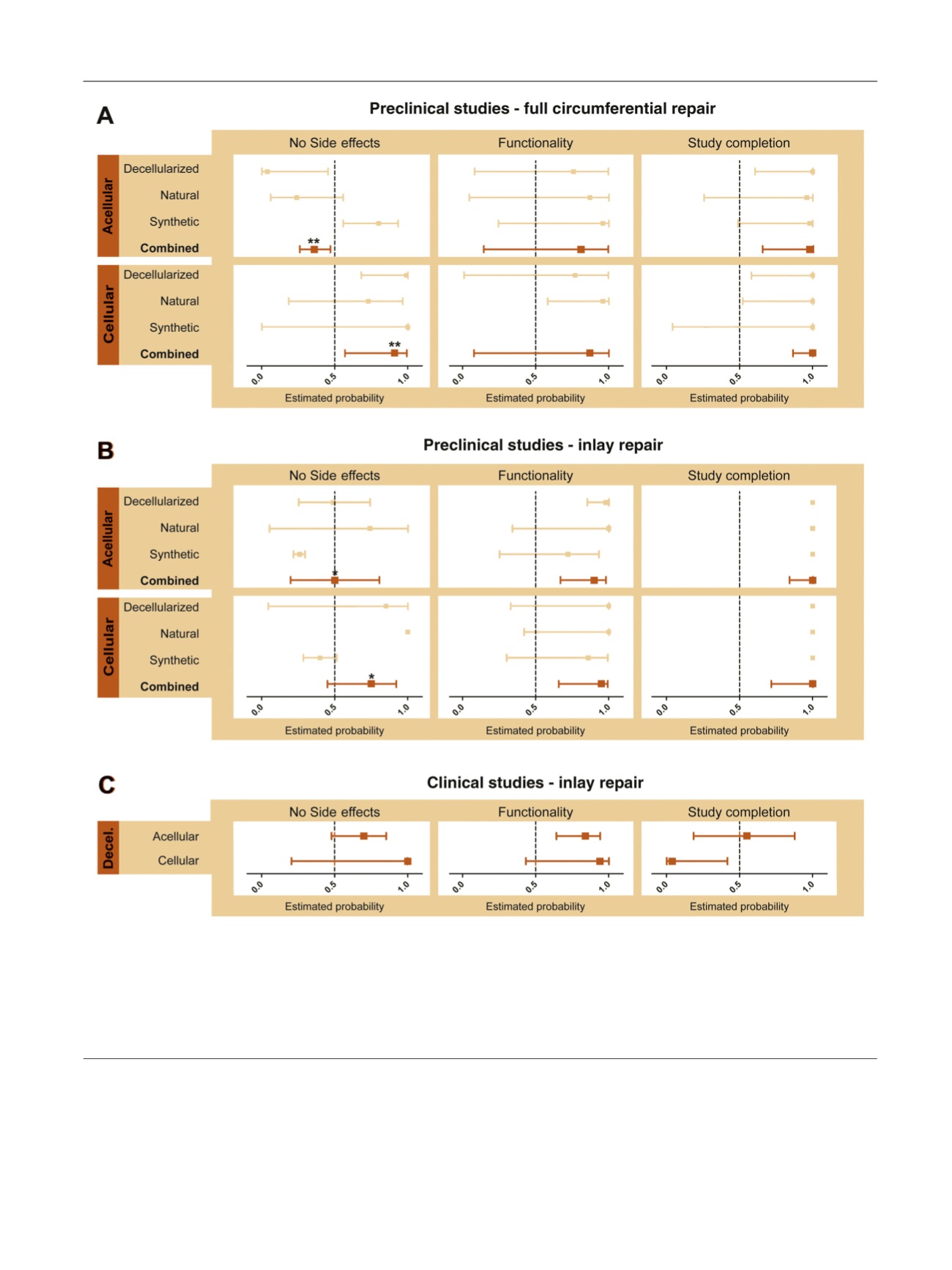
[(Fig._3)TD$FIG]
Fig. 3 – Estimated probability including 95% confidence intervals for the absence of side effects, functionality and study completion for (A) full
circumferential repair and (B) inlay repair in preclinical studies, both categorized for the use of cells and the type of biomaterial. (C) For the clinical
studies, only decellularized material with or without cells could be analyzed. The effect of cells on the three outcome measures was calculated in
estimated probabilities. Overall differences for cellular versus acellular templates were determined for each outcome measure for both full and inlay
repair. Specific point estimates and confidence interval are given in Supplementary data 6.
Decel. = decellularized.
*
p
= 0.003.
**
p
= 0.001.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 5 9 4 – 6 0 6
603