















 587 656
587 656

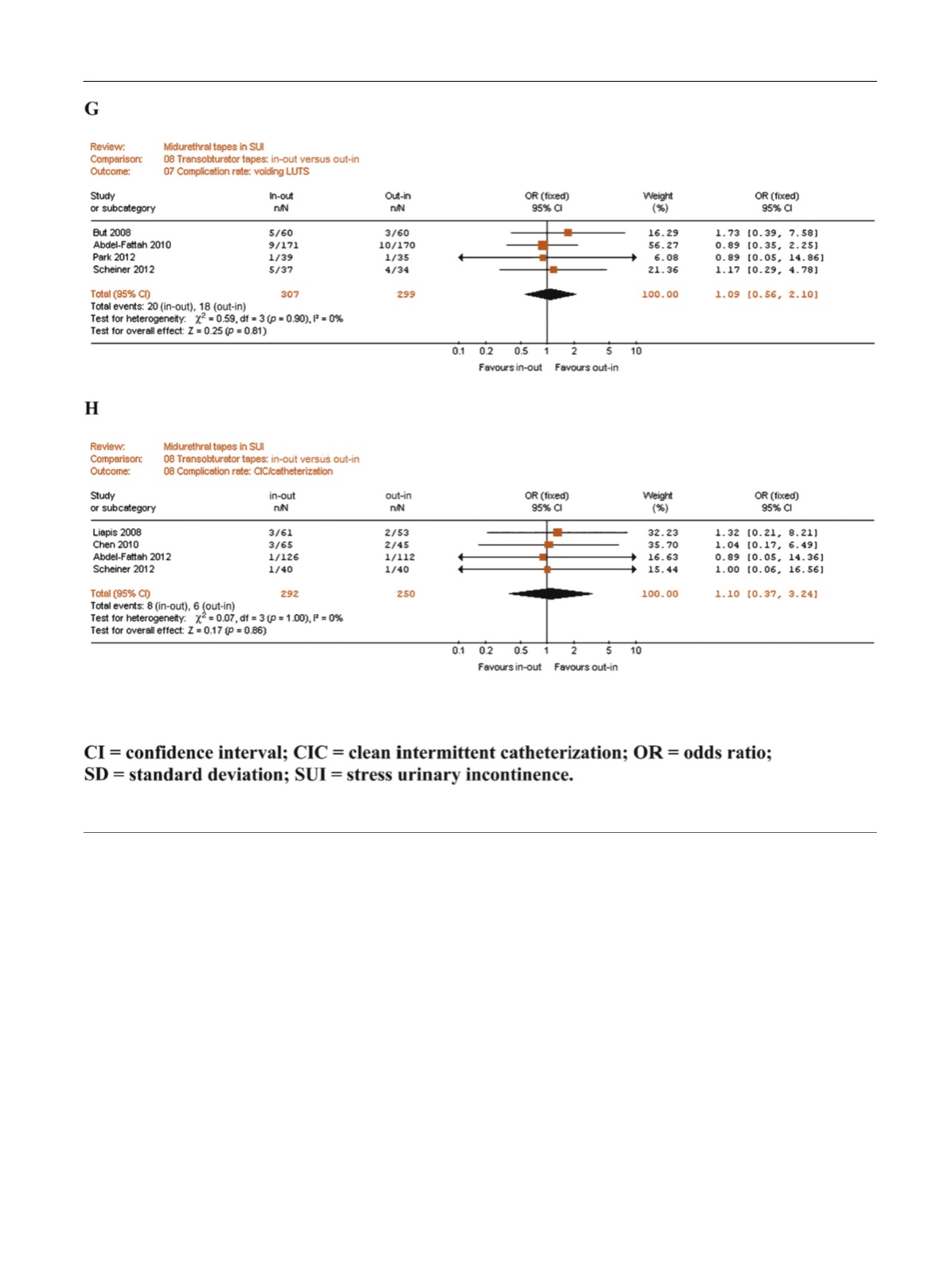
of inside-to-out TO-TVT (OR: 0.37,
p
= 0.06). All the other
complications were similarly prevalent inside-to-out
and outside-to-in TO-TVT. No RCT had a follow-up duration
60 mo.
3.5.
Publication bias
Funnel plots of all the studies used in this meta-analysis
were generated for all the evaluated comparisons. Only a
few studies lay outside the 95% CI with an even distribution
about the vertical, suggesting little evidence of publication
bias (data not extensively shown).
4.
Conclusions
Surgical treatment is the standard approach for women
with SUI who have failed conservative management
[45]. More than 200 surgical procedures have been
described over time. However, BC, PVS, and MUS are the
most popular and effective surgical treatments for woman
with SUI
[46]. To date, MUS represent the most frequently
used surgical intervention in Europe for women with SUI
[45]. Current European Association of Urology guidelines
recommend MUS in women with uncomplicated SUI as the
preferred surgical intervention and BC (either open or
laparoscopic) or autologous PVS in women with SUI if MUS
cannot be considered
[45]. In 2010, in a previous systematic
review and meta-analyses of RCTs evaluating the efficacy,
complication, and reoperation rates of MUS compared with
other surgical treatments for female SUI, Novara et al
[4]previously showed a statistically significant higher overall
and objective cure rates in favour of MUS compared with
BC, although at the cost of a statistically significant higher
risk of bladder and vaginal perforations. The comparison
[(_)TD$FIG]
Fig. 5. (
Continued
).
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 5 6 7 – 5 9 1
587