















 571 656
571 656

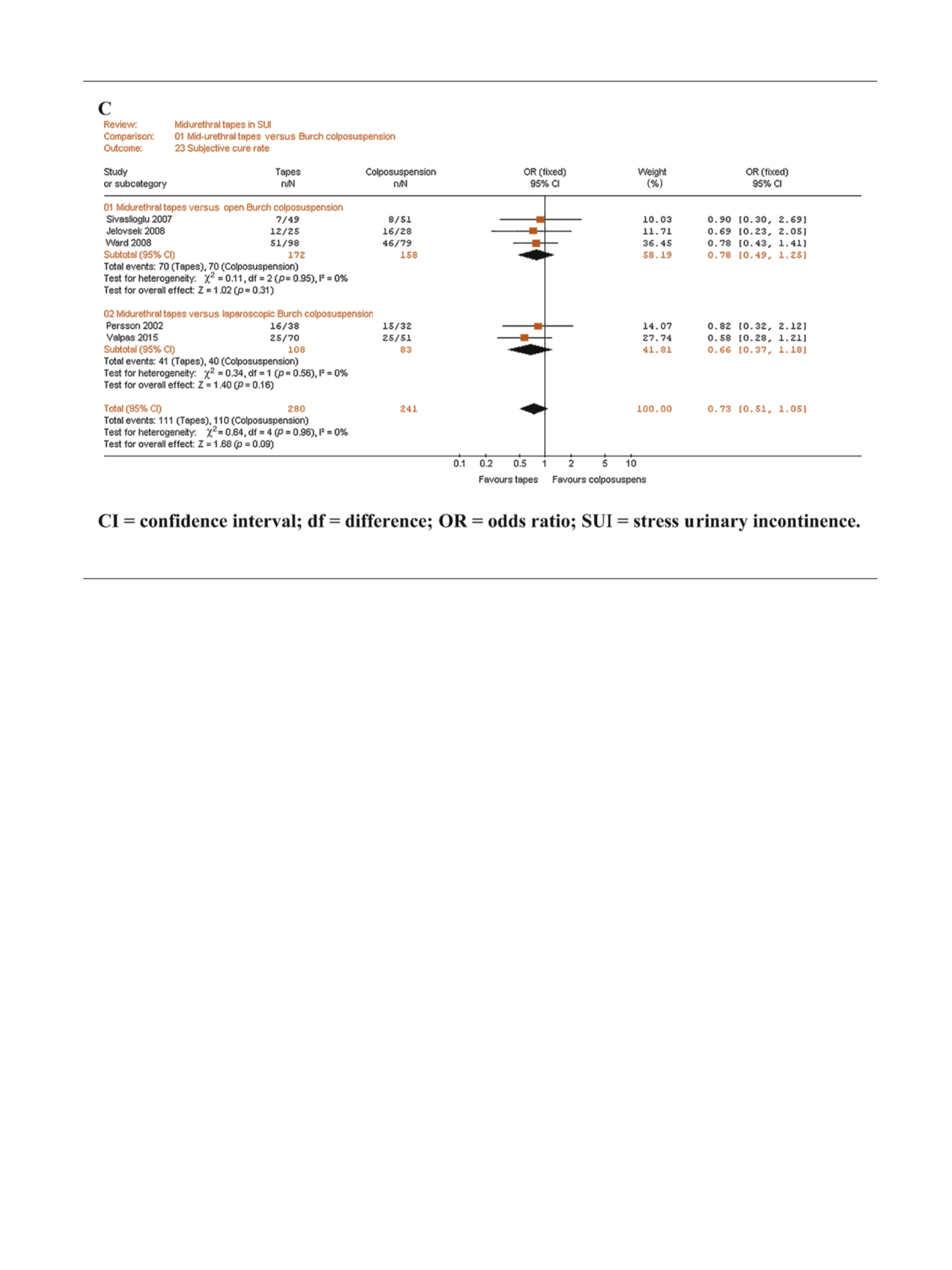
Subgroup analyses limited to the three studies with
follow-up duration 60 mo demonstrated better objective
cure rate for MUS (OR: 0.54, 95% CI: 0.36–0.82,
p
= 0.004)
but only a nonstatistically significant trend for overall
continence rate (OR: 0.39, 95% CI: 0.15–1.03,
p
= 0.06) and
subjective continence rate (OR: 0.69, 95% CI: 0.45–1.06,
p
= 0.09)
3.2.
RCTs comparing midurethral tapes with pubovaginal slings
Supplementary Table 2 summarises the results of the new
RCTs reporting continence and complication rates following
MUS or PVS as primary treatment for SUI.
Figure 3shows
the forest plots concerning the meta-analyses of cure and
complication rates.
On the whole, MUS and PVS were associated with similar
effectiveness and similar prevalence of complications.
However, there was there was some evidence of an effect
in favour of MUS for reoperation rates but it did not meet
conventional levels of statistical significance (3.9% vs 7.7%,
respectively, OR: 0.5,
p
= 0.06;
Fig. 3 G). Only one single RCT
had a follow-up duration 60 mo
[19].
3.3.
RCTs comparing retropubic with transobturator tape
Supplementary Tables 3 and 4 summarise continence,
complication, and reoperation rates of the RCTs comparing
RP-TVT and TO-TVT as ‘‘primary’’ treatment for SUI.
Figure 4shows the forest plots concerning the meta-analyses of
continence, complication, and reoperation rates.
Objective (86% vs 84%, respectively, OR: 0.82, 95% CI:
0.70–0.96,
p
= 0.01;
Fig. 4 B) and subjective (78% vs 74%,
respectively, OR: 0.83, 95% CI: 0.70–0.98,
p
= 0.03;
Fig. 4 C)
continence rates were superior in RP-TVT, whereas overall
continence rate was similar with RP-TVT and TO-TVT.
Considering ‘‘any definition of cure’’ there was no statistical
significance between RP-TVT and TO-TVT groups (OR: 1.16,
95% CI: 0.89–1.51,
p
= 0.27;
Fig. 4 A).
With regards to complications, risk of intraoperative
bladder or vaginal perforation (4.8% vs 1.6%, respectively,
OR: 2.4, 95% CI: 1.51–3.90,
p
= 0.0002;
Fig. 4D), pelvic
haematoma (1.7% vs 0.3%, respectively, OR: 2.61, 95% CI:
1.41–4.82,
p
= 0.002;
Fig. 4E), urinary tract infections (10%
vs 7.9%, respectively, OR: 1.31, 95% CI: 1.02–2.68,
p
= 0.04;
Fig. 4G), and voiding LUTS (9.2% vs 5.7%,
respectively, OR: 1.66, 95% CI: 1.2–2.3,
p
= 0.002;
Fig. 4I) were significantly higher in RP-TVT. Conversely,
the risk of vaginal erosion was lower in RP tapes (1.8% vs
2.8%, respectively, OR: 0.64, 95% CI: 0.44–0.92,
p
= 0.002;
Fig. 4F), which was mainly due to the higher risk of
vaginal erosions in outside-to-in TO-TVT. Finally, rates of
storage LUTS, clean intermittent self-catheterisation/
recatheterisation, and reoperation were similar in RP-TVT
and TO-TVT tapes.
Table 1summarises sensitivity analyses performed on
high quality RCTs. Such analyses reconfirmed advantages
for RP-TVT in terms of objective cure rates (OR: 0.76,
p
= 0.006) and risk of vaginal erosions (OR: 0.56,
p
= 0.03),
whereas bladder/vaginal perforations were less prevalent
with TO tapes (OR: 1.41,
p
= 0.002).
Further sensitivity analyses limited to the five RCTs
with follow-up durations
>
60 mo
[21,34,37–39]demon-
strated similar outcomes for RP-TVT and TO-TVT in terms
of objective cure rate, subjective cure rate, vaginal
[(_)TD$FIG]
Fig. 2. (
Continued
).
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 5 6 7 – 5 9 1
571