















 569 656
569 656

institutional questionnaires, or open interview) were
considered. In the case of papers reporting patient outcomes
through the use of mixed subjective and objective end points
(eg, no referred leakage and negative stress test, no referred
leakage, and negative pad test), an overall continence rate
was shown. Whenever multiple reports at different follow-
up duration were available for a RCT, the figures from the
reports with longest follow-up were considered.
Meta-analysis was conducted using Review Manager
software version 4.2 (Cochrane Collaboration, Oxford, UK).
Specifically, statistical heterogeneity was tested using the
chi-square test. A value of
p
<
0.10 was used to indicate
heterogeneity. In the case of a lack of heterogeneity, fixed-
effects models were used for the meta-analyses. The results
were expressed as weighted means difference and standard
deviations for continuous outcomes and as an odds ratio
(OR) with a 95% confidence interval (CI) for dichotomous
variables. In the comparisons of RP-TVT and TO-TVT, the
large number of publications with appropriate data allowed
us to perform subgroup analyses according to the device
used. In this case, we differentiated retropubic TVT versus
inside-to-out trasobturator (TVT-O), retropubic TVT versus
outside-to-in TO tapes (including different kits) and other
retropubic vs other transobutaror tapes (reporting studies
where either retropubic tapes different from TVT were used
or studies where both inside-to-out and outside-to-in TO
tapes were used without differentiating the results). No
covariate adjustments were performed, as usually done in
the Cochrane collaboration systematic reviews of RCTs.
For all the comparisons, sensitivity analyses limited to
RCTs of good methodological quality (ie, those with a Jadad
score 3) and to RCTs with follow-up duration 60 mo
were performed. The presence of publication bias was
evaluated through a funnel plot, as previously reported
[13]. The study complied with the recently reported
Preferred Reporting Items for Systematic Reviews and
Meta-analyses statement
[14].
3.
Evidence synthesis
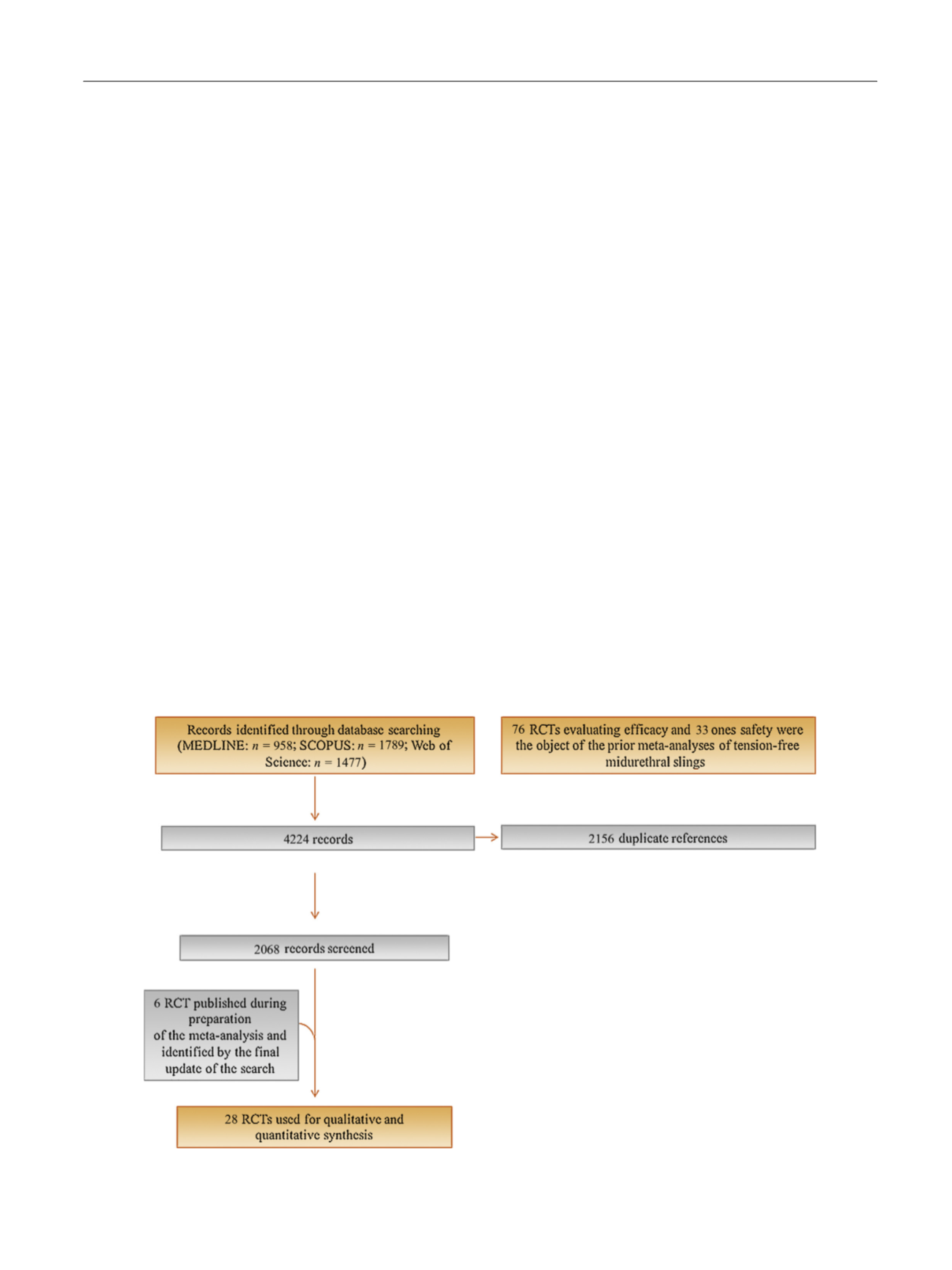
Figure 1summarises the literature review process which
lead to the identification of the 30 papers reporting data
from 28 different RCTs used to update the meta-analysis
( Fig. 1 ).
Specifically, two papers compared MUS and BC
[15,16] ;three papers compared MUS and PVS
[17–19]; 20 papers
compared RP-TVT and TO-TVT
[20–39]; two papers com-
pared RP-TVT and two different types of TO-TVT
[40,41] ;three studies compared different TO-TVT
[42–44]. Seventeen
reports were from 15 high-quality RCTs
[16,19,21–25, 27–29,32–34,38,41–43]. Only seven RCTs reported outcomes
of surgery at a follow-up interval 60 mo
[16,19,21,34, 37–39]. In total, the meta-analyses included 15 855 patients.
3.1.
RCTs comparing midurethral tapes to BC
Supplementary Table 1 summarises the results of the only
two new RCTs reporting continence and complication rates
following MUS or BC as primary treatment for SUI. Of note,
all BCs in these two new RCTs had been performed
laparoscopically.
Figure 2shows the forest plots concerning the meta-
analyses of continence rates following MUS or BC. MUS were
associated with significantly higher cure rates compared
[(Fig._1)TD$FIG]
Fig. 1 – Flow diagram of the systematic review and meta-analysis.
RCT = randomised controlled trial.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 5 6 7 – 5 9 1
569