















 486 656
486 656

Author contributions:
Quoc-Dien Trinh had full access to all the data in
the study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design:
Seisen, Sun, Trinh.
Acquisition of data:
Seisen, Sun, Leow.
Analysis and interpretation of data:
Seisen, Sun, Lipsitz, Abdollah,
Harshman, Nguyen, Bellmunt, Choueiri, Trinh.
Drafting of the manuscript:
Seisen, Sun, Lipsitz, Trinh.
Critical revision of the manuscript for important intellectual content:
Seisen,
Sun, Lipsitz, Abdollah, Leow, Menon, Preston, Harshman, Kibel, Nguyen,
Bellmunt, Choueiri, Trinh.
Statistical analysis:
Seisen, Lipsitz.
Obtaining funding:
None.
Administrative, technical, or material support:
None.
Supervision:
Bellmunt, Choueiri, Trinh.
Other:
None.
Financial disclosures:
Quoc-Dien Trinh certifies that all conflicts of
interest, including specific financial interests and relationships and
affiliations relevant to the subject matter or materials discussed in the
manuscript (eg, employment/affiliation, grants or funding, consultan-
cies, honoraria, stock ownership or options, expert testimony, royalties,
or patents filed, received, or pending), are the following: Firas Abdollah
has received consulting/advisory fees from GenomeDx. Adam S. Kibel
has received consulting/advisory fees from Dendreon, Sanofi, Tokai
Pharmaceuticals, MTG Biotherapeutics, and Profound Medical. Paul L
Nguyen has received consulting/advisory fees from Medivation, Abbott
Laboratories, GenomeDx, Ferring Pharmaceuticals, and Nanobiotix; and
holds an interest in a patent on volatile diagnostics for infections.
Joaquim Bellmunt has received consulting/advisory fees from Pierre
Fabre, Astellas Pharma, Pfizer, Merck, Genentech, and Novartis;
institutional research funding from Millennium Pharmaceuticals and
Sanofi; and travel/ accommodation expenses from Pfizer and MSD
Oncology. Toni K. Choueiri has received honoraria from the National
Comprehensive Cancer Network and UpToDate; consulting/advisory
fees from Pfizer, Bayer AG, Novartis, GlaxoSmithKline, Merck, Bristol-
Myers Squibb, Genentech, Eisai, Prometheus Labs, Foundation Medicine
Research, Cerulean Pharma, AstraZeneca, and Peloton Therapeutics; and
institutional research funding from Pfizer, Novartis, Merck, Exelixis,
TRACON Pharmaceuticals, GlaxoSmithKline, Bristol-Myers Squibb,
AstraZeneca, Peloton Therapeutics, and Genentech. Thomas Seisen,
Maxine Sun, Stuart R. Lipsitz, Jeffrey J Leow, Mani Menon, Lauren C
Harshman, and Quoc-Dien Trinh have nothing to disclose.
Funding/Support and role of the sponsor:
None.
Acknowledgments:
The data used in the study are derived from a
deidentified NCDB file. The American College of Surgeons and the
Commission on Cancer have not verified and are not responsible for the
analytic or statistical methodology employed, or the conclusions drawn
from these data by the investigators. Quoc-Dien Trinh is supported by an
unrestricted educational grant from the Vattikuti Urology Institute, a
Clay Hamlin Young Investigator Award from the Prostate Cancer
Foundation, and a Genentech BioOncology Career Development Award
from the Conquer Cancer Foundation of the American Society of Clinical
Oncology.
Appendix A. Supplementary data
Supplementary data associated with this article can be
found, in the online version, at
http://dx.doi.org/10.1016/j. eururo.2015.12.049.
References
[1]
Ploussard G, Daneshmand S, Efstathiou JA, et al. Critical analysis of bladder sparing with trimodal therapy in muscle-invasive bladder cancer: a systematic review. Eur Urol 2014;66:120–37.[2]
Paramasivan S, Huddart R, Hall E, Lewis R, Birtle A, Donovan JL. Key issues in recruitment to randomised controlled trials with very different interventions: a qualitative investigation of recruitment to the SPARE trial (CRUK/07/011). Trials 2011;12:78.[3]
Bekelman JE, Handorf EA, Guzzo T, et al. Radical cystectomy versus bladder-preserving therapy for muscle-invasive urothelial carcino- ma: examining confounding and misclassification bias in cancer observational comparative effectiveness research. Value Health 2013;16:610–8.[4]
Smith AB, Deal AM, Woods ME, et al. Muscle-invasive bladder cancer: evaluating treatment and survival in the National Cancer Data Base. BJU Int 2014;114:719–26.[5]
Gofrit ON, Nof R, Meirovitz A, et al. Radical cystectomy vs. chemor- adiation in T2-4aN0M0 bladder cancer: a case-control study. Urol Oncol 2015;33, 19.e1-5.[6]
Austin PC. An introduction to propensity score methods for reduc- ing the effects of confounding in observational studies. Multivariate Behav Res 2011;46:399–424.[(Fig._1)TD$FIG]
0
20
40
60
80
100
Trimodal therapy
Radical cystectomy
Overall survival (%)
0
120
108
96
84
72
60
48
36
24
12
Time
(
mo
)
p
<
0.001
0
20
40
60
80
100
(A)
(B)
0 12 24 36 48 60 72 84 96 108 120
Trimodal therapy
Radical cystectomy
Overall survival (%)
Time
(
mo
)
p
<
0.001
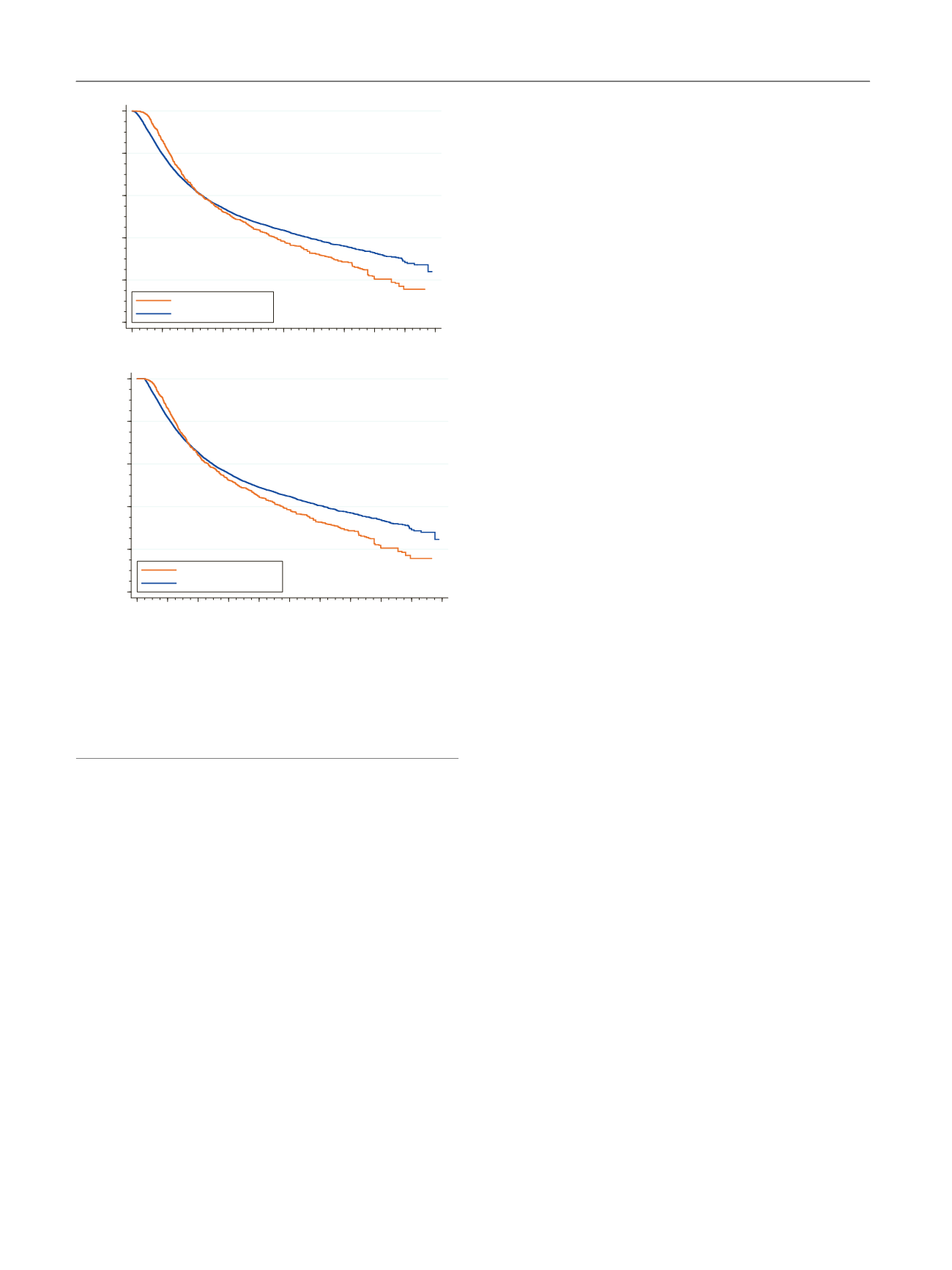
Fig. 1 – Inverse probability of treatment weighting (IPTW)–adjusted
Kaplan-Meier analysis of overall survival (A) without and (B) with a 3-
mo conditional landmark in patients who received trimodal therapy
versus radical cystectomy for localized muscle-invasive urothelial
carcinoma of the bladder. The
p
values were calculated using a
x
2
test
from an IPTW-adjusted Cox regression model with a time-varying
covariate for comparison of trimodal therapy versus radical cystectomy.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 4 8 3 – 4 8 7
486